AI Video Analytics in Hospitals: Patient Safety, Elopement Detection and HIPAA-DPDP Compliance in India
Improve Patient Safety With Real-Time AI Video Analytics Using Existing CCTV Infrastructure.
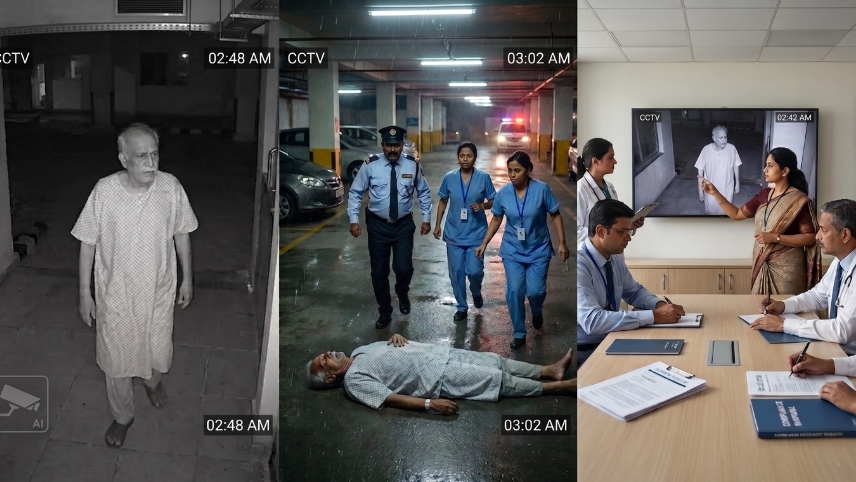
A geriatric patient with moderate dementia is admitted to a 400-bed hospital for a hip fracture. At 2:47 AM on day three, he wanders out of his ward, takes the service stairwell, and is found two floors below by a cleaning crew forty minutes later. The cameras captured every step. Nobody was watching.
This is not a security failure. The cameras worked. The footage exists. What failed was the layer between recording and response. The system that should have generated a 2:47 AM alert instead produced a 3:28 AM discovery.
An AI video analytics system for healthcare in India is not a CCTV upgrade. It is the answer to a clinical question that has quietly become a compliance question too: what happens to a hospital when passive surveillance is no longer enough? Modern healthcare AI surveillance systems transform passive camera networks into active patient safety infrastructure.
Hospitals Are High-Risk Environments That Passive CCTV Was Never Designed For
Most hospital CCTV deployments were designed for one purpose: recording evidence in case something goes wrong. That purpose has not changed. What has changed is the understanding of what "going wrong" looks like in a clinical environment and how quickly it happens.
Three patient populations create specific monitoring requirements that do not exist in manufacturing, warehouses, or any other environment this technology is typically deployed in:
- Dementia and cognitive impairment patients - India is estimated to have 8.8 million people living with dementia, based on a 2023 nationwide study published in Alzheimer's and Dementia journal. As this population ages into hospital and elder care settings, the risk of unsupervised wandering and elopement becomes a direct clinical liability, not just an operational inconvenience.
- Psychiatric in-patients - Research consistently shows that the highest-risk window for patient absconding is within 48 hours of admission. A passive recording system that captures the departure and stores it for review does nothing to prevent what happens in the forty minutes before anyone notices.
- Pediatric patients - Unauthorized removal from neonatal wards and pediatric units is a documented risk that requires zone-level access monitoring, not perimeter cameras pointed at the main entrance.
AI surveillance in hospitals does not replace clinical staff. It gives them eyes in places and at hours where a nurse-to-patient ratio cannot sustain continuous physical monitoring.
Elopement Detection: The Clinical Safety Use Case Most Indian Hospitals Are Not Monitoring
Elopement in a hospital context means the unauthorized departure of a patient from a supervised clinical area without the knowledge or consent of clinical staff. It is not the same as a planned discharge. It is a dementia patient navigating a fire exit at 3 AM. A psychiatric inpatient walking out through a service corridor during a shift handover. An elderly post-surgical patient attempting to "go home" while still medically unstable.
The consequences range from patient injury to patient death, with significant medico legal liability attached to each outcome.
AI video analytics systems for healthcare address elopement specifically through the following capabilities:
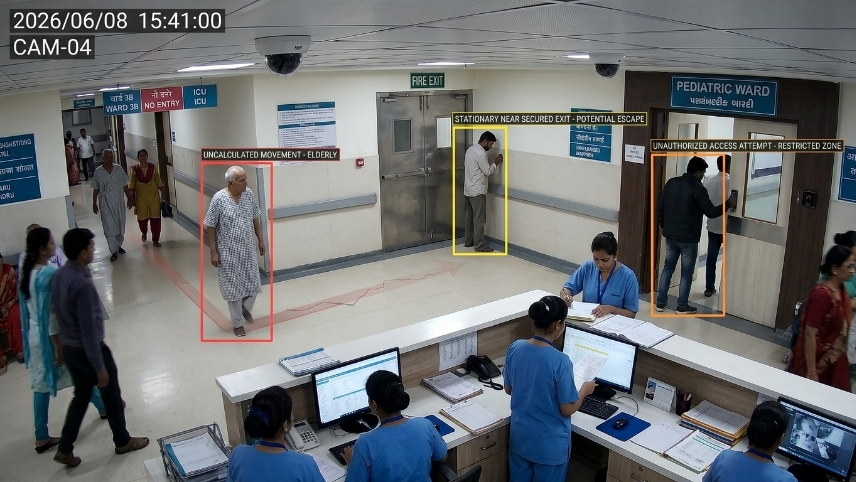
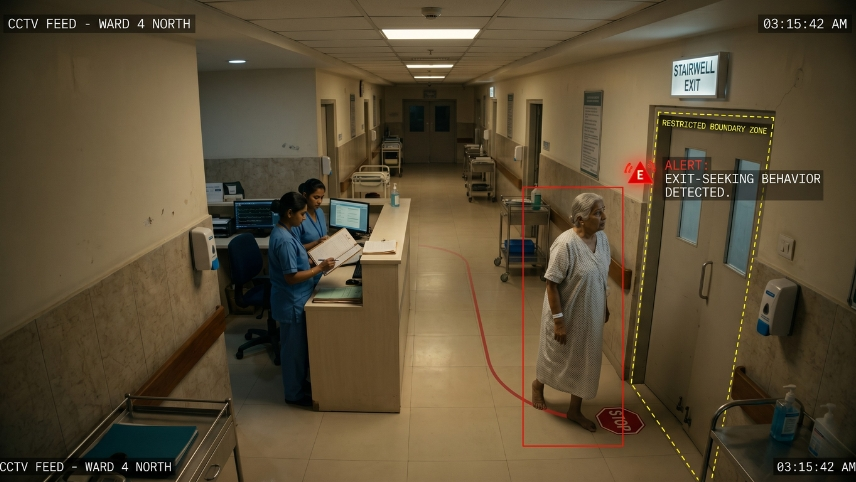
- Exit-seeking behavior detection - The system identifies patients moving toward restricted exits, service stairwells, or ward perimeter zones at atypical hours and generates a real-time alert to the nursing station before the patient leaves the monitored area. The intervention window exists. Passive CCTV discards it.
- Zone boundary alerts for flagged patient categories - Specific wards and egress points are configured as restricted for patients with documented wandering risk. Any movement toward those boundaries triggers an immediate alert rather than waiting for the next nursing round.
- Night shift and shift transition coverage - Most elopements occur during low-staffing periods when nursing rounds are less frequent. AI monitors these windows continuously without a headcount dependency.
- Fall detection within the elopement pathway - Fall detection is one of the most valuable AI patient safety applications because it reduces response times during critical incidents. A patient who wanders and then falls in a corridor, stairwell, or bathroom generates a separate alert before anyone discovers them. The two events are clinically distinct and both require immediate response.
Elopement is a sentinel event under most hospital accreditation frameworks. It triggers mandatory reporting, internal review, and in serious cases, regulatory scrutiny. The monitoring system that prevents it is not a luxury deployment. It is patient safety infrastructure.
Patient Safety Monitoring Beyond Elopement
The same camera infrastructure that enables elopement detection supports a broader set of clinical safety use cases. None of these require separate hardware deployments.
AI surveillance systems in hospitals covers:
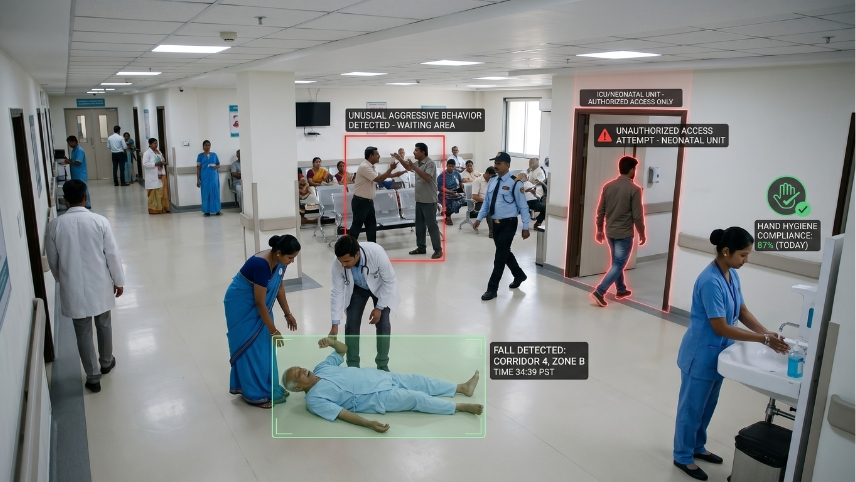
- Fall detection in patient rooms and corridors - When a patient goes to the floor, an alert goes to nursing staff immediately. The current standard in most Indian hospitals is discovery at the next nursing round or by another patient. That delay matters clinically.
- Restricted zone access monitoring - ICU, neonatal unit, pharmacy, blood bank, and operating theater corridors all carry unauthorized access risks. AI monitors these zones continuously without stationing security personnel at every door.
- Hand hygiene compliance monitoring - In infection-sensitive zones, AI can track whether staff are using hand hygiene stations at clinically required intervals. Relevant for hospital-acquired infection control, particularly in post-surgical and intensive care settings.
- Violence and aggression detection in high-risk areas - Emergency departments and psychiatric wards carry documented staff safety risks. Behavioral anomaly detection that generates an alert before an incident escalates gives security personnel a response window.
- Code response documentation - AI timestamps every event from detection to staff arrival, creating an automatic audit trail for clinical governance, NABH accreditation, and incident reporting purposes.
Smart hospital surveillance enables continuous monitoring of high-risk clinical environments without increasing staff workload. These capabilities do not require a hospital to build separate surveillance systems for each use case. One deployment. One infrastructure. Multiple clinical applications.
Your CCTV cameras recorded it. Your staff found out an hour later.
That gap is not a security problem.
It is a clinical safety problem.
Book a Free Demo with Mikshi AIHIPAA vs DPDP: What Indian Hospitals Actually Need to Know
Many Indian hospital compliance teams search for HIPAA guidance when evaluating surveillance systems. The reason is understandable. HIPAA is the most widely referenced global health data standard, and hospitals with international patient programs or US healthcare partnerships encounter it regularly. But HIPAA is a US law. It is not the operative framework for Indian hospital surveillance compliance.
What HIPAA says about video surveillance, briefly: HIPAA does not explicitly regulate CCTV systems. Under the HIPAA Security Rule, any system capturing identifiable patient information must be protected with access controls, retention policies, and breach notification protocols. Useful context. Not Indian law.
What the DPDP Act 2023 actually requires: The Digital Personal Data Protection Act 2023 is India's operative data protection legislation. For hospitals, it creates specific obligations that directly govern how surveillance footage of patients is managed:
- Video footage of identifiable patients is personal data - under the DPDP Act. Its collection, storage, and use is subject to the Act's requirements.
- Explicit consent - is required before processing patient personal data beyond direct clinical care. Footage used for operational analytics, vendor sharing, or quality reporting requires documented consent.
- Data minimization - Only footage necessary for the stated purpose should be retained. Indefinite retention of all CCTV footage without a defined policy is not compliant.
- Breach notification - If surveillance footage is accessed without authorization, the hospital must notify the Data Protection Board of India. Penalties reach up to Rs 250 crore for failure to implement reasonable security safeguards.
- Cross-border transfer restrictions - Patient footage stored on overseas servers requires compliance with the Act's data transfer provisions. This is a direct implication for cloud-first platforms with no India-resident deployment option.
The DPDP Act is not fully enforced yet with the scheduled deadline being May 14, 2027 for the final phase of implementation. The Data Protection Board of India is operational. The enforcement framework is maturing. Hospitals that build compliant surveillance infrastructure now will not need to retrofit it under regulatory pressure later.
What DPDP-Compliant Hospital AI Surveillance Looks Like in Practice

Understanding the obligation is one thing. Evaluating whether your platform meets it is another. Before deploying any AI video analytics system for healthcare in India, verify:
- On-premise deployment option - Cloud-only platforms routing patient footage through overseas servers create an immediate cross-border transfer compliance question. On-premise or India-resident cloud deployment resolves it.
- Configurable retention periods - Clinical safety footage from a psychiatric ward has different retention requirements from general corridor footage. The platform must support both.
- Access controls and audit logs - Every footage access must be logged with who, when, and for what purpose. This is what a DPDP compliance audit will ask for.
- Vendor compliance documentation - Any AI surveillance vendor processing patient footage is a data processor under the DPDP Act. The hospital as data fiduciary is responsible for that vendor's compliance posture. Get documentation in writing.
As AI healthcare technologies become more common, hospitals are increasingly using video analytics to improve safety and operational oversight. Mikshi AI supports on-premise, cloud, and hybrid deployment with configurable retention and access controls built for regulated environments.
What One Elopement Incident Actually Costs an Indian Hospital
Consider what follows a preventable elopement event. A patient with dementia leaves a ward undetected at night, sustains a fall in the parking lot, and is found an hour later with a fracture. Internal clinical governance review is mandatory. The family files a complaint. A Consumer Forum complaint follows under the Consumer Protection Act 2019. NABH assessors flag it as a sentinel event requiring root cause analysis. Legal counsel is retained.
Direct cost of the legal and management response: conservatively Rs 10 lakh to Rs 30 lakh depending on severity and legal proceedings. Reputational cost does not appear on a balance sheet but does appear in bed occupancy numbers when the incident reaches local media or patient review platforms.
The AI surveillance system that generates a 2:47 AM alert costs a fraction of the liability from a single incident it fails to catch. That is not a safety argument dressed in financial language. It is an accurate description of what Indian hospital administrators face when a preventable safety event occurs and the monitoring gap is documented. AI CCTV analytics for hospitals can identify exit-seeking behavior, restricted zone movement, and wandering patterns before a patient leaves a supervised area.
Patient Safety Is the Argument. Compliance Is the Obligation.

Improving hospital safety requires more than recording incidents; it requires identifying risks and alerting staff before harm occurs. AI video analytics system for healthcare in India serves two purposes simultaneously. It closes the clinical gap between a camera recording and a clinical response. And it creates the documented monitoring trail that the DPDP Act now requires hospitals to maintain.
These are not two separate technology decisions. They are the same deployment serving both the patient safety team and the compliance function simultaneously
The hospitals that build this now are not just protecting patients from elopement, falls, and unauthorized access. They are building the compliance architecture that the Data Protection Board of India will increasingly expect to see as enforcement matures, and the clinical governance documentation that NABH review processes already require.
AI surveillance in hospitals is a clinical tool with a compliance obligation wrapped around it.
In this article
- Hospitals Are High-Risk Environments That Passive CCTV Was Never Designed For
- Elopement Detection: The Clinical Safety Use Case Most Indian Hospitals Are Not Monitoring
- Patient Safety Monitoring Beyond Elopement
- HIPAA vs DPDP: What Indian Hospitals Actually Need to Know
- What DPDP-Compliant Hospital AI Surveillance Looks Like in Practice
- What One Elopement Incident Actually Costs an Indian Hospital
- Patient Safety Is the Argument. Compliance Is the Obligation.





